
Guidance on Conducting Peer Audits or Self-Audits: Class II nuclear facilities and prescribed equipment
Guidance on Conducting Peer Audits or Self-Audits: Class II nuclear facilities and prescribed equipment (PDF, 0.50 MB)
Preface
During inspections, staff at the Canadian Nuclear Safety Commission (CNSC) have observed a common trend among the various Class II facilities of failing to comply with certain regulations and licence conditions. These non-compliances are mainly associated with licensees not following or not updating the policies and procedures referenced in their licence. A simple audit of the licensee’s program performed either internally or by a peer could help remedy these non-compliances before they negatively impact the safe operation of the facility. Additionally, if the peer audit or self-audit were completed frequently and effectively, the non-compliances found could be addressed so that they did not come up in CNSC inspections. Frequent audits would also indicate whether the program is working effectively and facilitate continuous improvement in performance. Furthermore, the audit results would be a useful tool for communicating the facility’s performance to the radiation safety committee and the applicant authority.
It is important to note that this program will not be effective unless the applicant authority, the radiation safety officer and senior management are on board and fully support its implementation.
Table of Contents
1. Introduction
1.1 Purpose
In recognizing the numerous benefits of peer audits and self-audits, the Canadian Nuclear Safety Commission (CNSC) has created this guide to aid licensees in establishing their own peer- or self-audit programs.
1.2 Scope
This guidance document defines peer audits and self-audits and outlines the steps for conducting such audits at licensees’ facilities.
1.3 Definitions
A peer audit is an audit conducted by cross-functional audit team members from another facility / other facilities who have no direct responsibility in the work/process being audited, thereby ensuring objectivity. The peer audit is a more formal assessment whereby the audit typically determines the extent of compliance of a process or department with an organization’s procedures or standards or regulatory requirements. A peer audit may also recommend areas of improvement based on lessons learned from the audit team members’ own experiences, but the main focus is to determine compliance with regulatory requirements that have to be met, rather than self-established performance targets.
A self-audit is an audit conducted by internal multidisciplinary team members to determine the extent of compliance with the organization’s policies and procedures or regulatory requirements. Although a self-audit may also recommend areas of improvement, the main focus is to determine compliance with regulatory requirements that have to be met.
2. Procedure
A peer- or self-audit program consists of four cyclical steps:
2.1 Plan
The first step is to establish the frequency and scope of the audits. The frequency and scope should depend on the complexity, risk and range of licensed activities. Because a large facility may need more than one audit to fully examine their program, in which case the scope of licensed activities covered by each audit should be broken down into manageable sizes.
Next, it would be beneficial to create a baseline plan for the audits based on the defined frequency and scope. An optimal plan would have audits completed prior to internal desktop reviews of policies and procedures, as well as CNSC inspections.
For example, a licensee who operates five medical linear accelerators (linacs) and a cyclotron could plan to perform audits at the beginning of each year for the linacs and halfway through the year for the cyclotron.
It is critical that the plan be flexible and changeable in relation to the performance of licensed activities. For example, if there is an unexpected increase in radiation doses to workers, the frequency of audits should be increased and the plan updated accordingly until the doses return to as low as reasonably achievable.
2.2 Prepare
2.2.1 Plan logistics
As the audit approaches, determine the exact dates for the audit and the resources required.
If planning a peer audit, arrange with a peer from outside the department or from another facility to conduct the audit. Provide the peer with the scope of audit and all relevant information on facility operations.
2.2.2 Assemble team
When choosing a team, consider a multidisciplinary team made up of members with varying levels of experience and different roles within the program. A multidisciplinary team will ensure that all aspects of licensed activities are examined from multiple perspectives that will lead to achievable, effective and sustainable improvements. The size of the team should be commensurate with the scope of the audit. The CNSC recommends the following team composition by sector:
| Sector | Team members |
|---|---|
| Medical | Radiation safety officer |
| Medical physicist | |
| Medical radiation technologist | |
| Service engineer | |
| Industrial | Radiation safety officer |
| Operator | |
| Service engineer | |
| Commercial | Radiation safety officer |
| Service engineer | |
| Radiopharmaceutical technician | |
| Academic and research | Radiation safety officer |
| Operator |
For a peer audit, the team should consist of members who conduct licensed activities that are similar to those of the licensee being audited, or have an understanding of these licensed activities.
2.2.3 Define criteria
A list of requirements from applicable regulations and the facility’s licence should be compiled by the audit team, accompanied by detailed expectations on how each requirement is met at the facility.
An example of the criteria used by the CNSC while conducting inspections is provided as guidance in the table at the end of this document.
The scope of the audit does not have to be limited to CNSC requirements, but can also be an opportunity to include other activities important to the facility (e.g., quality assurance activities for patient safety).
2.2.4 Review
The final step before execution is for the audit team to familiarize themselves with all relevant aspects of the licensed activities and to review any previous audit results. This will allow the audit team to readily identify any non-compliance(s) that may have been noted in previous findings.
2.3 Execute
The fundamentals of executing an audit are to collect evidence, analyze the evidence for findings, and develop corrective actions or recommendations to address the findings.
2.3.1 Collect evidence
Evidence is collected by reviewing records and observing licensed activities.
2.3.1.1 Records review
Review a representative sample of all applicable records since the last audit was performed. The following are examples of records to be reviewed:
- nuclear energy workers’ designations
- service records
- safety system tests
- training records
- dosimetry results
- calibration records of radiation survey meters
- leak test results (if applicable)
- incidents or events
When reviewing records, ensure each record is complete and populated in accordance with the policies and procedures referenced in the licence. Document any discrepancies or opportunities for improvement found in the records.
2.3.2 Observation of licensed activities
Observe licensed activities being conducted. This should include:
-
a walk-through of the facility to verify correct installation of:
- safety systems
- security systems
- appropriate signage and postings
- inventory checks of sealed sources (if applicable)
- observation of safety system testing
- observation of other applicable procedures referenced in the licence (e.g., contamination control)
2.3.3 Develop findings and corrective actions
Analyze all the evidence (facts) collected during the audit. If there are multiple facts proving that criteria for the same regulatory requirement or program element have not been met, this evidence can be concluded as a finding. If there are two or more findings similar in nature, a corrective action or recommendation should be developed to address the findings.
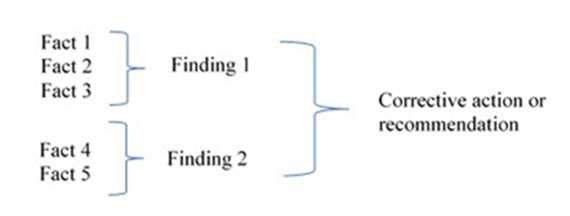
Figure 2 – Text version
This is an example of how a corrective action or a recommendation is developed. Three different facts make up a first finding. Two other different facts make up a second finding. Both findings form the basis for a corrective action or a recommendation.
The corrective action or recommendation should be SMART (specific, measurable, achievable, relevant and time bound). The deliverables should be clear with specific closure criteria. This can be easy for prescriptive requirements (like posting a sign), but more difficult for performance-based expectations. An example of a performance-based corrective action is as follows:
The [institution name] shall implement measures to ensure that all staff receive appropriate safety training by January 1st, 2019. This shall include:
- development of safety awareness training for security and housekeeping staff
- revision of existing training material to address changes in facility operations
- completion of training for security and housekeeping staff, and refresher training for all staff
For a peer audit, the peer should provide the licensee with their audit findings and suggested corrective actions. It is the licensee’s responsibility to close out the audit.
2.4 Close out
2.4.1 Discuss results
The radiation safety officer (RSO) should discuss the audit results with all staff and management involved in the licensed activities that were audited. The results should also be discussed by the radiation safety committee. During discussions, the RSO should ensure that the corrective actions are agreed upon, and should highlight strengths and areas for improvement in operations. Lessons learned from the audit process should also be shared.
This discussion with staff will enhance the facility’s safety culture by valuing the contributions of workers to safety performance, and by reinforcing the value and priority of safety. In addition, the discussion will increase the RSO’s visibility within the facility, making the workers more comfortable with raising safety issues.
Moreover, the RSO should discuss the audit with the applicant authority and ensure that the applicant authority agrees with the closure of corrective actions. This is important, as the applicant authority is ultimately accountable for ensuring that the licensee operates safely.
2.4.2 Document audit results
Finalize the corrective actions and recommendations based on feedback from staff and management, and document them in a report along with a description of the evidence, the findings, and strengths uncovered during the audit.
2.4.3 Implement corrective actions
Create an action plan for implementing the corrective actions or recommendations. Ensure the following is defined in the plan for each action: detailed closure criteria, individual responsible for implementing the action, and the due date.
Here is an example of closure criteria for the corrective action example above: Revised training program documentation and training records demonstrate completion of all required training.
The RSO should track all actions until completion and verify their effectiveness.
3. Conclusion
Implementing a peer- or self-audit program can result in substantial improvements in the facility’s safety performance, security and safety culture, as well as a better compliance record with the CNSC. If licensees ever need help with peer audits or self-audits, they should not hesitate to contact their respective project officer at the CNSC.
Appendix
Table 1: Example criteria for CNSC Type II inspection
| Safety and control area: Fitness for service | ||||
|---|---|---|---|---|
| Regulations or licence condition | Item | Expectations | Evidence | Evaluation |
| CII 15(13), 21(2)(c) | Servicing safety systems |
Verify that:
|
Observations: |
Compliant? ☐ Yes ☐ No |
| Records: | ||||
| Safety and control area: Human performance management | ||||
| Regulations or licence condition | Item | Expectations | Evidence | Evaluation |
| GN 12(1)(a), 12(1)(b); CII 3(q), 4(s), 21(2)(b); TDG 6.6, 6.7 | Responsibilities, qualifications and training of workers | Verify that training records are kept and include the date of the training, the trainee's name and the topic. | Observations: |
Compliant? ☐ Yes ☐ No |
| Records: | ||||
| Safety and control area: Physical design | ||||
| Regulations or licence condition | Item | Expectations | Evidence | Evaluation |
| CII 15(2) | Door interlock, last-person-out btn |
Verify that:
|
Observations: |
Compliant? ☐ Yes ☐ No |
| Records: | ||||
GN:
General Nuclear Safety and Control Regulations
CII:
Class II Nuclear Facilities and Prescribed Equipment Regulations
TDG:
Transportation of Dangerous Goods Regulations
Page details
- Date modified: